And now a subtle variation from ECG number 4
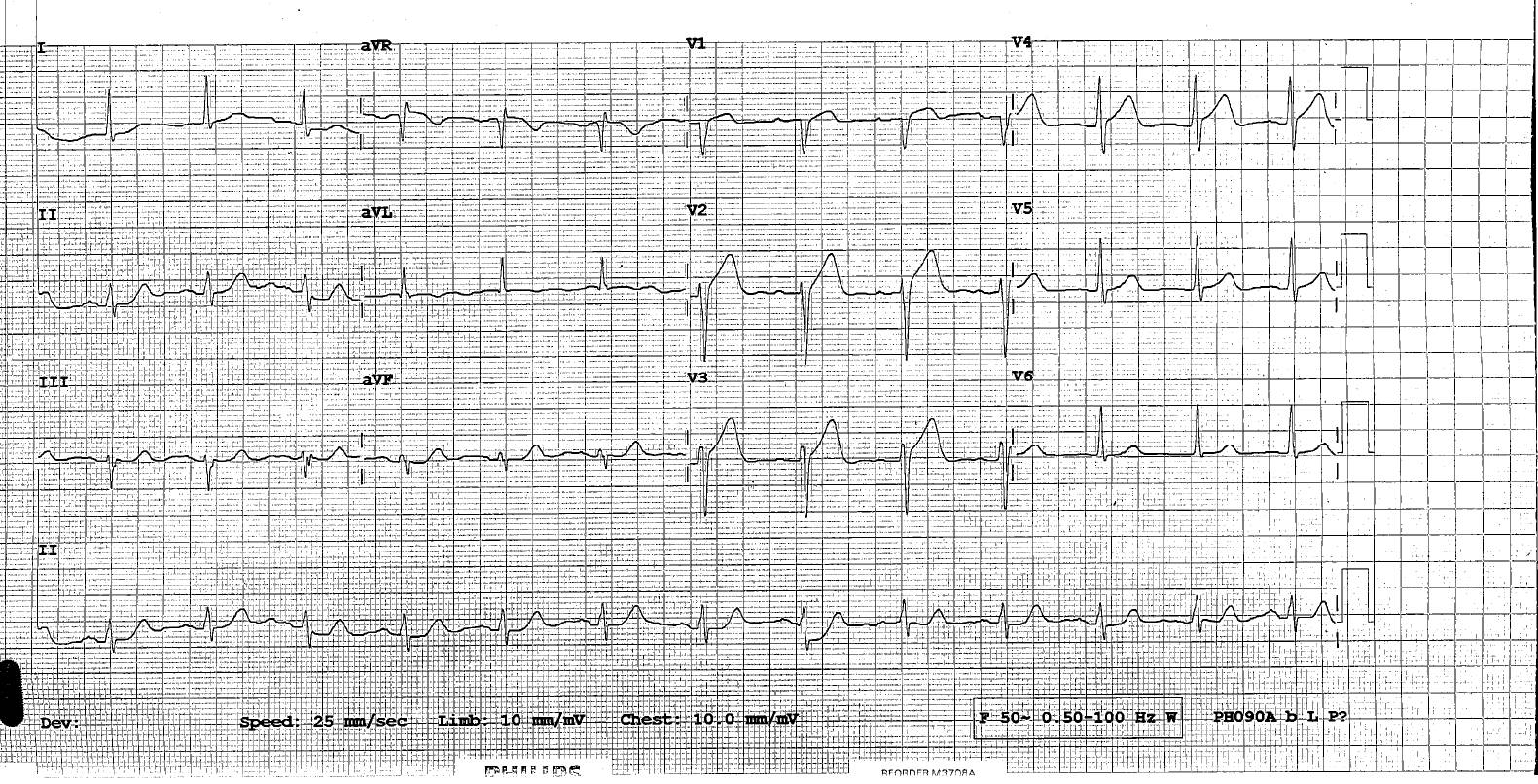
A 45 year old male smoker comes with with 1 hour of moderate central chest pain.
What are the key features of this ECG?
What would you do next?
click on ECG to enlarge
And now a subtle variation from ECG number 4
click on ECG to enlarge






1 Comment
Hi all
The obvious feature of concern here is the concave ST elevation in the septal leads. It extends from V1 -V4 and is not associated with reciprocal changes elsewhere.
This is a classic Ischaemic STE vs benign early repolarization ECG.
.
BER would classically have <25% STE height vs TWave height, is often <2mm in total and can include other leads also.
.
This ECG leans towards the ischaemic side of the ledger as V1 looks convex and the STE: TW ration is >25%.
.
My preference is to call the interventionalist and discuss it ASAP. I advocate for cath if there is a good story and new change or no prior ECG. This man had an 100% prox LAD at angio.
.
Some of you may have noticed some minor ST elevation in aVR and be thinking rightly about Proximal L main stenosis with this finding. Classically an acute L main AMI with STE in aVR will have ST depression in the septal leads also but it does not have to. Generally STE in aVR should be greater than 0.5mm and greater than the STE in V1 to be persuasive. If present it correlates with higher rates of LMCA disease and higher adverse 90 day event rates including death. In this ECG it adds to your concern level without absolutely meeting criteria on its own