Posted by Nick Taylor on August 6, 2015 at 6:00 am
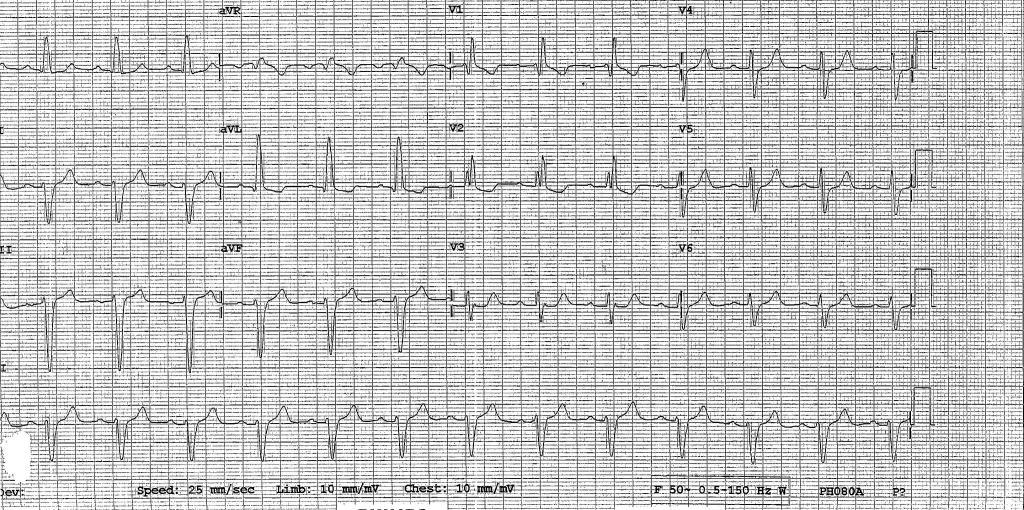
So this ECG is sinus rhythm and has broad complexes with RSR’ in V1 V2 consistent with RBBB. the PR interval is over 200ms (1 big square) so there is a first degree AV block as well.
There is also a left axis deviation (V1 up aVF down).
In the setting of RBBB and Left axis you should think about left anterior or posterior hemi/fascicular block (LAFB, LPFB).
There are rS complexes in II, III, aVF and qR complexes in I and aVL; so this is a left anterior fascicular block.
So there is a fair bit of poor conduction: all of the Right bundle, half the left bundle and enough of the AVNode/proximal His to give a long PR.
This is known as a trifascicular block (although isnt really 3 fascicles)
Not suprisingly, this amount of delay for your p waves to translate into meaningful LV contraction may be an issue.
How much of an issue??
The concern is development of 3rd degree AV Block (Complete Heart Block) which in someone with AV nodal disease only will probably lead to an okay life preserving junctional escape rhythm.
But, if your conduction problem is because your entire bundle of His (and probably thus, also your Left Ventricle) is buggered, then 3rd AVB escapes with an ineffective ventricular escape and you fall over and possibly die.
In Electrophysiology land the goal is to determine if the block is in the AV node or in the sub nodal bundle (more worrying because of that poor escape clause)
Framingham said that chances of progression of trifascicular block to 3rd degree AV block was about 1-3% per year
So in non EP land
If you have a history of syncope or you have a very bad LV function and you have a trifascicular block on ECG you should get a pacemaker.
This lady from the fall at the pub should get a pacemaker if her conduction issues arent reversible (eg too much Calcium blocker).




0 Comments
You can be the first one to leave a comment.